You must have an order with a minimum of $150.00 to place your order, your current order total is $0.00.
Product Pillars, Peptide Education, Research Protocols
TB-500: Complete Research Guide to Thymosin Beta-4 Peptide

22
May
May
Research Use Only Notice: TB-500 is a research peptide intended for in-vitro and animal research applications only. It is not FDA-approved as a drug or therapy. Nothing in this article constitutes medical advice, treatment recommendation, or guidance for human consumption.
TB-500 is the synthetic peptide version of thymosin beta-4 — a naturally occurring 43-amino-acid peptide found throughout human and animal tissues. Research on TB-500 spans cardiac repair, dermal wound healing, corneal injury, and broader cell migration biology. The compound has been a focal point of tissue-repair research for decades, with substantial published literature documenting its actin-binding mechanism and downstream effects. This complete guide from the chemistry team at OPS Peptide Science walks through what TB-500 is, how it works in research models, where it sits in the broader research catalog, and how it pairs with BPC-157 in combination protocols.
For the foundational research-workflow protocols this guide assumes, see our companion guides on how to reconstitute peptides, how to inject peptides, and peptide storage and refrigeration.
What Is TB-500?
TB-500 is the synthetic, research-grade version of thymosin beta-4 (TB-4) — a 43-amino-acid peptide naturally produced in nearly all human and animal tissues. The “500” designation refers to the research nomenclature, not a fragment number — TB-500 is the full-length thymosin beta-4 sequence, synthesized for laboratory use.
Key facts about TB-500:
- Chemical class — 43-amino-acid peptide, synthetic version of naturally occurring thymosin beta-4
- Molecular weight — approximately 4963 Da
- Source — synthesized to match the natural human thymosin beta-4 sequence
- Form — typically supplied as lyophilized (freeze-dried) powder; reconstituted with bacteriostatic water for research administration
- Half-life — longer than most small peptides due to tissue binding; effective biological half-life is measured in days rather than hours
- Stability — stable at -20°C as lyophilized powder for 18-24 months; reconstituted solutions stable for 21-28 days refrigerated
Unlike many research peptides, TB-500’s natural counterpart (thymosin beta-4) is one of the most abundant peptides in mammalian cells, present at high concentrations in platelets, tissues, and circulating plasma. This means TB-500 research has a robust foundation in the natural biology of the compound — researchers know what the molecule does because cells use it for actin regulation and repair as a normal function.
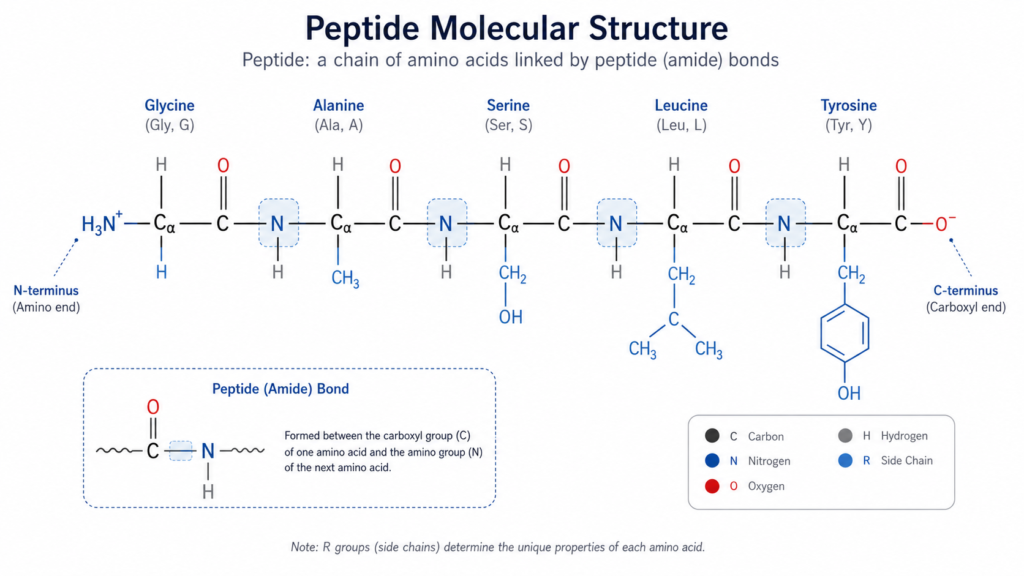
TB-500 Structure and Chemistry
The TB-500 / thymosin beta-4 sequence is one of the most characterized small peptides in cell biology research. Key structural features:
- 43 amino acids — longer than most synthetic research peptides, which sit in the 5-15 amino acid range
- Actin-binding domain — the central functional region that gives the peptide its primary biological activity
- N-terminal acetylation — naturally occurring in human thymosin beta-4; synthetic TB-500 typically reproduces this modification for stability
- Highly conserved across species — the thymosin beta-4 sequence is nearly identical across mammals, supporting cross-species research translation
The actin-binding domain is what makes TB-500 functionally interesting — it’s not a hormone analog targeting a single receptor, but a cytoskeletal modulator influencing cell shape, migration, and tissue organization at the structural level.
How TB-500 Works in Research (Mechanism)
The TB-500 mechanism is among the better-characterized of research peptides. Documented activities:
- G-actin sequestration — TB-500 binds free G-actin monomers, regulating the dynamic balance between G-actin and F-actin (filamentous actin)
- Actin polymerization control — by controlling G-actin availability, TB-500 influences when and where actin filaments form, which determines cell shape and movement
- Cell migration regulation — fundamental to tissue repair, where cells must migrate to injury sites
- Anti-inflammatory effects — independent of actin binding, TB-500 has been documented to modulate inflammatory pathways
- Angiogenesis support — research has measured effects on endothelial cell migration and new blood vessel formation
- Stem cell activation — published research documents effects on progenitor cell activity in repair contexts
The actin biology mechanism is what gives TB-500 its broad research applications. Almost any tissue repair process involves cell migration, and cell migration requires actin reorganization — which TB-500 directly influences. The thymosin beta-4 tissue repair literature on PubMed documents the mechanism across hundreds of studies.
TB-500 Research Applications
The research literature on TB-500 covers several major application areas:
Cardiac Research
One of the most extensively studied TB-500 applications is in cardiac injury research. Animal models of myocardial infarction have documented measurable effects on cardiac tissue repair, reduced scar tissue formation, and improved heart function endpoints in TB-500-treated subjects. This research extended to clinical trials in some countries (though TB-500 remains non-FDA-approved in the US).
Dermal Wound Healing Research
Skin injury models — burn, surgical wound, diabetic ulcer — show accelerated re-epithelialization, improved granulation tissue quality, and reduced scarring in TB-500-treated research subjects. The compound’s effects on cell migration directly support the wound-healing process at the cellular level.
Corneal Research
Ocular research includes corneal wound healing models, dry eye research, and corneal epithelial regeneration studies. TB-500 has documented effects on corneal repair markers across multiple animal research models.
Musculoskeletal Research
Tendon, ligament, and muscle injury research uses TB-500 to study cell migration during repair. The published research overlaps with BPC-157 research in this area, though the mechanisms are distinct — BPC-157 works through VEGF and angiogenesis, TB-500 works through actin and cell migration.
Hair Follicle Research
A smaller but documented research area on TB-500 effects on hair follicle stem cells and follicle activity. Animal models have measured changes in follicle cycling and stem cell markers.
TB-500 Dosing in Research Models
TB-500 dosing in published research models has distinct features compared to shorter peptides:
- Less frequent dosing — TB-500’s effective biological half-life supports less frequent administration than short-half-life peptides; twice-weekly or weekly protocols appear in published research
- Larger absolute dose ranges — because the peptide is larger (43 aa vs. 15 aa for BPC-157), research doses tend to be larger in mg amounts
- Subcutaneous or intramuscular — both routes documented in published research; SC is more common
- Tissue depot effects — TB-500 binds tissues and produces effects beyond what acute plasma levels would predict, complicating simple pharmacokinetic interpretations
Research protocols should reference published methodology for the specific research model. Tissue-binding behavior means TB-500 dosing protocols require careful design — single doses can produce extended effects, while frequent dosing may not produce proportional additive responses.
TB-500 Storage and Stability
TB-500 stability profile aligns with most lyophilized research peptides:
| Storage Condition | Form | Stability Window |
|---|---|---|
| -80°C (ultra-low freezer) | Lyophilized powder | 3-5+ years |
| -20°C (standard lab freezer) | Lyophilized powder | 18-24 months |
| 2-8°C (refrigerated) | Lyophilized powder | 6-12 months |
| Room temperature | Lyophilized powder | 2-4 weeks for transit |
| 2-8°C (refrigerated) | Reconstituted in BAC water | 21-28 days |
For practical storage protocols, see our companion guide on how long do peptides last at room temperature. Larger peptides like TB-500 (vs. smaller compounds like BPC-157) sometimes show slightly different oxidation susceptibility — protocols that work for both compounds generally cover TB-500 safely.
TB-500 + BPC-157 Combination Research (Wolverine Stack)
One of the most-discussed research applications is the combination of TB-500 with BPC-157 — popularly called the Wolverine Stack in research and biohacking discussions. The rationale:
- Different mechanisms — TB-500 acts on actin and cell migration; BPC-157 acts on VEGF, angiogenesis, and multiple signaling pathways
- Different half-lives — TB-500’s tissue-binding gives extended effects; BPC-157’s shorter half-life allows acute signaling
- Potentially complementary — TB-500 supports the cell migration phase of repair; BPC-157 supports the angiogenesis and inflammation modulation phases
- Documented in published research — both compounds appear in combination protocols across animal tissue-repair studies
Research design for combination studies requires separate reconstitution, alternating injection sites, and careful documentation of each compound’s contribution to the endpoint. The Wolverine Stack name is informal — published research literature uses BPC-157 + TB-500 terminology — but the combination protocol is real and documented. See our overview on peptides for healing and recovery for the broader context.
How to Identify Quality TB-500
TB-500’s larger size (43 amino acids vs. 15 for BPC-157) makes it more challenging to synthesize cleanly. Quality criteria for research-grade TB-500:
- 99%+ purity confirmed by HPLC-MS analysis — synthesis of longer peptides produces more degradation products; purity verification is especially important
- Per-lot Certificate of Analysis — each batch independently tested with full chromatographic profile
- Mass spectrometry identity confirmation — confirms the molecular weight matches TB-500 (4963 Da), distinguishing from shorter degradation products
- Chain-of-custody documentation — traceable from manufacturer through fulfillment
- Properly lyophilized appearance — clean white cake at the bottom of the vial, no discoloration or moisture damage
- Research-use-only labeling — required by US regulations
At OPS Peptide Science, every TB-500 vial ships with a unique BIOVIRIDIAN COA code. Customers can verify the Certificate of Analysis for their specific lot — confirming the full HPLC-MS purity report and identity verification before opening the vial.
TB-500 Regulatory Status
TB-500 / thymosin beta-4 occupies a specific position in US regulatory frameworks:
- Not FDA-approved — has not completed clinical trials required for human drug approval in the US
- WADA-prohibited — listed under category S2 (peptide hormones, growth factors, related substances), banned in and out of athletic competition
- Legal as research chemical — sold in the US for in-vitro and animal research under research-use-only labeling
- Not DEA-scheduled — no controlled substance status
- Some clinical research history — has been studied in clinical trials internationally for cardiac and dermal indications, though not FDA-approved
For the complete legal framework around research peptides like TB-500, see our detailed guide on are peptides illegal. According to NIH research literature, TB-500 remains an active pre-clinical research compound across multiple tissue-repair applications.
FAQ
What is TB-500?
TB-500 is the synthetic, research-grade version of thymosin beta-4 — a 43-amino-acid peptide naturally produced in nearly all human and animal tissues. It is one of the most-studied tissue-repair research peptides, with substantial published literature documenting effects on cardiac, dermal, corneal, and musculoskeletal injury models.
Is TB-500 the same as thymosin beta-4?
Yes — TB-500 is the synthetic research-grade version of thymosin beta-4. The two names refer to the same compound, with “TB-500” being the research nomenclature and “thymosin beta-4” being the biological name. Some sources also use “TB4” as a shorthand.
Is TB-500 legal in the US?
TB-500 is legally sold in the US as a research chemical for in-vitro and animal research, under research-use-only labeling. It is not FDA-approved for human use. WADA has prohibited it in athletic competition.
How long does TB-500 stay in the body in research?
TB-500’s plasma half-life is short, but its biological half-life is much longer due to tissue binding. Effective effects in research models can extend for several days after a single dose — longer than the plasma half-life would suggest. This is why TB-500 research protocols often use less frequent dosing (twice-weekly or weekly) than shorter peptides.
What’s the difference between BPC-157 and TB-500?
Both are tissue-repair research peptides, but they act through different mechanisms. BPC-157 (15 amino acids) acts on VEGF, angiogenesis, and multiple signaling pathways. TB-500 (43 amino acids) acts on actin sequestration and cell migration. They are often combined in research protocols (the Wolverine Stack) because the mechanisms complement rather than overlap.
How is TB-500 administered in research?
Most published TB-500 research uses subcutaneous injection. Intramuscular injection also appears in some research protocols. Less frequent dosing schedules (twice-weekly or weekly) are common due to TB-500’s tissue-binding properties and extended biological half-life. See our complete guide on how are peptides administered for context across administration routes.
Where can I buy research-grade TB-500?
Research-grade TB-500 is sold by research peptide suppliers operating under research-use-only labeling. Quality criteria include 99%+ HPLC-MS verified purity, per-lot Certificates of Analysis, mass spectrometry identity confirmation, and traceable chain-of-custody. Browse the OPS Peptide Science catalog for verified research-grade TB-500.
TB-500 (thymosin beta-4) stands out among research peptides for its mechanistic clarity, its broad tissue-repair research applications, and its strong pairing with BPC-157 in combination protocols. For researchers studying tissue repair, cell migration, cardiac biology, or dermal endpoints, TB-500 is one of the most-cited compounds in the modern research catalog.
For research-grade TB-500 backed by per-lot Certificates of Analysis and full HPLC-MS purity documentation, browse the OPS Peptide Science catalog, visit the OPS Peptide Science homepage for the full product overview, or verify a specific lot using its COA code.
Author: Shane Straight, Principal Chemist, OPS Peptide Science
Reviewed: May 2026